How intention constellations can bring clarity
Franz Ruppert
Abstract
Instead of using the abstract term "health condition", it is better to talk about "being healthy". As a psychotherapist, you can ask yourself: How does it turn out that a person is mentally healthy? What promotes freshness and what hinders it? Disease is a construct that can lead to only the symptoms being treated. This simplistic approach means that the real cause of the symptoms, which lies deeper, is often obscured. Many symptoms are the result of a trauma. They may be an immediate expression of a trauma, or they may stem from attempts to repress the trauma. "Traumatized love" and "traumatized sexuality" are forms of traumatization that have a profound impact on people's lives. It can lead to many kinds of symptoms of illness, both physical, psychological and social. Intention constellations are a method developed by the author. This method makes use of basic knowledge from multigenerational psychotraumatology and helps clients to become mentally healthy and to stabilize their healthy state.
Being mentally healthy
It has long been known that good health is not the same as the absence of disease (Fröschl 2000). Good health also does not automatically come when disease symptoms are removed. In any case, it is more clarifying to talk about being healthy. It is an expression of the way one lives one's life, not an abstract description.
We psychotherapists also need a separate theoretical concept that defines what it means to be mentally healthy. Orienting yourself using categories such as DSM or ICD is not enough to work therapeutically with people so that they really get well and stay well. On the contrary, categorization of mental disorders often leads to people becoming even more mentally ill than they were before. A diagnosis such as schizophrenia or borderline syndrome (emotionally unstable personality disorder, alt. definition according to the ICD-10 manual) can be a violation of a person's sense of self, and such diagnoses can promote a desire to give up so that one stops striving for to return to a healthy existence.
The basis of my psychotherapeutic work is a concept of mental health which includes ideas by Dan Siegel. All mental functions, which involve registering reality in a meaningful way and selecting relevant information and processing it further, must fit well together. The energy that drives the psychic programs to process the information further must be able to flow freely. The information must become a meaningful whole. According to Dan Siegel, a healthy psyche is full of energy, and it is stable, integrated, coherent and complexly organized. It is neither too rigid nor too flexible, it is maximally open to new things without ending in chaos (Siegel 2010, p. 352 f.).
Trauma is the source of many physical and psychological symptoms
In general, I assume that psychological abnormalities are consequences of psychological traumatization, especially when the disorders are chronic. This means that in order to become mentally healthy, the person must integrate traumatizing life experiences into the psyche, and people who live in traumatizing environments must detach themselves from them.
The knowledge and insight that I have gained through 20 years of practice as a psychotherapist have turned into a theory of multigenerational psychotraumatology. I have presented the basis for this concept in my previous books (Ruppert 2001, 2002, 2005, 2007, 2010, 2012, 2014).
According to this theory, there are in principle three states a living organism can be in:
- A healthy state (well-being). The person does not feel threatened and can therefore be open to his surroundings, while at the same time he can set boundaries around himself in a good way.
- A stressed state. Man is threatened by dangers. The entire organism is activated and focused to prevent harmful influences. These are stress reactions.
- A traumatizing condition. Humans (or other organisms) are exposed to threats from the outside world. These are too strong for you to protect yourself with a stress reaction, it will rather worsen the situation. The chance of survival increases if the highly activated stress reaction is calmed down. For that to happen, important psychic functions must be blocked: the sensations must be switched off, the emotions must be frozen, the thoughts must be stopped and one must not act. When this happens, the inner wholeness and coherence, the psychic integration, is destroyed.
Persistent stress, experiencing continuous threats, is one of the main sources of physical and psychological symptoms. This has major social consequences. Stressed people have problems in relationships, and they find it easy to provoke conflicts between people.
Persistent stress is, according to my model, a significant consequence of the psyche splitting after a traumatic experience. It is therefore the result of a trauma. A person with traumatic experiences also runs a greater risk of acting in ways that lead to new traumatic experiences. This happens partly because repressing these experiences can make the person in question unable to see reality, and partly because the person concerned will create illusions that they see as reality, and in that way will be able to harm themselves.
After a traumatic experience, a person has three different active programs in his psyche (see picture 1):
- Programs that still represent the trauma situation, despite the fact that the external circumstances have changed (traumatized parts)
- Programs intended to keep the severed, traumatized parts out of consciousness (survival strategies)
- Programs that, despite the trauma experience, are healthy (healthy parts)
The splitting of the structure of a living organism after a traumatic experience

Image 1: The splitting of the structure of a human after a traumatic experience.
After many years of psychotherapeutic experience, for me a healthy psyche has the following characteristics:
- The sensations are open to the realities.
- The feelings are adapted to the external and internal reality, i.e. they can be regulated from within.
- The thoughts are oriented towards truth and clarity.
- The own identity is clear and defined.
- You remember important experiences.
- Own possibilities are assessed in a realistic way.
- Relationships with others are constructive and are terminated if they become destructive.
People with trauma experience have, next to their healthy parts, two more psychic structures:
- An emotional fire torch, that is. the psychological experience of the trauma.
- A firefighter trying to put out the fire, or at least trying to prevent the fire from starting again.
I call this the survival parts.
According to my theory, these two psychic structures contain everything that can manifest as symptoms.
When the traumatized structures are activated, one can, for example, feel panic through symptoms such as palpitations, disturbances in heart rhythm, diarrhoea, abnormal sweating, digestive problems, uncontrolled aggressiveness or bottomless grief and despair.
The survival strategies, which are in a permanent state of stress to keep the traumatized parts under control, produce countless symptoms themselves:
- They add to the pain and confusion that distracts.
- They contribute to the consumption of medicines and drugs to anesthetize themselves even more.
- They contribute to physical overexertion, which causes premature wear and tear on the body, and mental and physical overexertion, which leads to burnout.
There is a whole catalog of symptoms that are classified as illness in the diagnostic tool DSM V. These symptoms are, by and large, nothing more than a list of the many different survival strategies that people use to keep their traumatized structures under control. A smaller part of the diagnoses in DSM V refer directly to traumatized parts (for example panic disorder).
My experience is that the symptoms that come from traumatized structures and from survival strategies are characterized by the type of traumatization involved. In my theory, I distinguish between different forms of trauma.
There are two main types
- shock trauma, i.e. a sudden trauma
- relationship trauma
We experience shock trauma, for example, in a car accident or when a person we love dies suddenly. Relational trauma, on the other hand, is long-lasting, for example in a couple or a parent-child relationship.
Another categorization in my theory distinguishes between four traumas
- existential trauma
- loss trauma
- symbiosis trauma
- attachment system trauma
Traumas of existence and loss usually generate states of shock. For existential and loss traumas, I have already mentioned some examples.
Symbiosis and attachment system trauma are different forms of relational trauma and often burden people throughout their lives. A symbiotic trauma occurs when a child fails to have a vital, secure attachment to his mother and a stable and supportive attachment to his father. No matter how hard the child tries, all attempts fail because the parents are traumatized. They are unable to create the emotional contact that the child needs in order to have a stable psychological development.
I focus particularly on the attachment between mother and child, because the mother is the first person the child bonds with. It already happens before birth. All other affiliations come after that. This also applies to the connection between father and child. It can be very emotional, but is always subordinated to the influence of the quality of attachment between mother and child. This is also the case if the father makes contact with the child already during the pregnancy. The mother's special role must also find its expression in the theory. Experience from psychotherapy shows that there are many more who struggle with a complicated relationship with their mother than with their father, despite the fact that the relationship with their father can be traumatic.
In the event of a symbiotic trauma, the relationship with the parents is turned upside down. The child is worried about the mother's well-being and uses all his strength and energy to stabilize his traumatized parents. The child does everything to get in touch with them. It even identifies itself with its parents' severed trauma parts and copies their survival parts.
An important consequence of the symbiosis trauma is that the child attaches himself to other people as a substitute for the mother when he cannot find a secure connection with her. It can also happen that the child tries to meet its symbiotic needs with the father instead of with the mother. If the father can meet the symbiotic needs, it is of great help to the child. But because traumatized mothers most often find themselves traumatized men, the child who is searching for a secure connection often goes from bad to worse.
In recent times, I have also begun to distinguish between different forms of traumatizing violence that we can be exposed to (see picture 2)
- traumatization due to natural forces
- traumatization due to human violence
- traumatized love
- traumatized sexuality
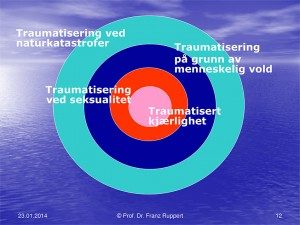
Image 2: Traumatization due to violence
Traumatized love corresponds to the concept of symbiosis trauma. The term love was brought in to clarify that it is about traumatizing the core of our human existence and our basic needs. When we cannot love, when we may never have learned what healthy love is, we have no prerequisites for healthy attachment and healthy interpersonal relationships. This has a strong impact on our enjoyment of life and on all the efforts we go through to be able to live in relationships, whether as couples, as families or in working relationships. In the case of traumatized love, our contact with other people is fundamentally disturbed, we either limit ourselves too much, we withdraw extremely and avoid contact or we commit abuse, lack respect for other people's boundaries and enter into a symbiosis with them.
Traumatized love is often the foundation for traumatized sexuality. When a child does not receive the important and necessary physical contact and emotional care from its mother, and in addition lacks protection, the child becomes easy prey for people who have a sexual interest in the child. Sexual abuse is often the result, and this has dire consequences for the child. Earlier I mentioned that particular physical symptoms can be linked to particular traumas. Anorexia is a possible consequence of sexual abuse, i.e. traumatized sexuality. My experience is that the symptom of anorexia often occurs in those who are exposed to sexual abuse
- because the child will make his body unattractive to the abuser
- because the child will gain control over the body's reactions so that the body will not react with desire when it becomes
- forced sexual stimulation
- because the child believes that it can live without its body
- because the child cannot talk about the sexual abuse, but still looks for recognition from the emotionally distant mother through achievements and success
Illness as construction
Headache, high blood pressure, cancer, fibromyalgia, rheumatism, anxiety, depression, dementia. The list of all physical and psychological symptoms that we label as illness is almost endless. And it keeps getting longer: The new edition of the Diagnostic and Statistical Manual of Mental Disorders, DSM V, is more comprehensive than its predecessor. For example, there is now a disease called disproportionate anger.
We are all used to thinking in disease categories, and it seems a matter of course, therefore it is also important to ask critical questions about the artificial construction "disease". In many cases it is, logically speaking, just an unnecessary repetition with new concepts. A phenomenon, such as a severe headache, becomes a disease term. This often happens using Latin or Greek names. One example could be migraine. What is written before and after the equal sign looks different (severe headache = migraine), but the words have the same content. The tautological equation of a symptom with a disease has several practical consequences:
- The cause of the symptom is not questioned.
- The symptom is recognized as illness and thus socially accepted.
- This recognition entails rights to receive medical treatment for the symptom.
- You get medical treatment that is paid for by the public.
All this is not objectionable in itself, but the method has a major and significant disadvantage: the symptoms are classified as illness, and therefore the treatment is also based on the symptoms. The doctor or psychotherapist who will treat the disease must, through their measures, remove the symptom completely, or at least reduce it so much that they are no longer disturbing.
When, for example, a young woman stops eating, and the disease that is diagnosed is eating disorders (anorexia nervosa), the treatment starts with motivating her to eat again or by forcibly supplying her body with nutrition. Although the young woman may put on weight in this way, it does not change the basic attitude she has towards herself. She still rejects her body. The treatment also does nothing to change the symbiotic entanglements within the family system which in all likelihood are the cause of the symptoms.
In any case, with constructed diseases, it is not about the sick person, but about the symptoms. When we as doctors, therapists or in another job in the healthcare system use the concept of disease, we have to ask ourselves another question: What are the causes of the symptoms that a person suffers from?
Why can one person have the same symptoms as another, but still not experience it as a disorder? What possible functions do the symptoms perform? What would have been present if the symptoms were no longer there? If so, was this person healthy?
The disease symptoms resulting from symbiotic entanglements
From my experience, symbiotic entanglements that are a consequence of trauma fuel many of the symptoms we see. In the case of love trauma, a child will bond with his traumatized mother with the help of the symptom. Despite the fact that the child suffers from the symptom, he is unable to let go of it. Then the child would also have given up contact with his mother.
After a sexual trauma, a person will find themselves in the victim/aggressor split. The person may suffer from many symptoms, but will not take a closer look at what they originate from. This may be because one would then have become aware of the extent of one's existence as a victim. Often, the victim of abuse still has a relationship with the abuser, a relationship that really should have ended. Then it is easier to escape into the symptoms or into a role as sick. The hope is that one can then prevent new abuses and at the same time be able to continue in the destructive relationship.
In the case of an attachment system trauma, it becomes most clear why the theory of psychotraumatology must be multigenerational. Some children are born into families steeped in victim/abuser relationships. In order to survive in such a system, the child has no other choice but to become a victim and/or abuser himself. Such children therefore develop victim and aggressor attitudes as a survival strategy. Only when a person steps out of such a relational system, can that person be freed from the victim/aggressor split that that person has within them. Only then can he or she aim for a life without victim and aggressor attitudes.
Constellations of intention
In 1994 I came into contact with the principle of family constellations via Bert Hellinger. He made the topic known through books and public events (Weber 1995). For a period I imitated Hellinger's way of working, but gradually I realized more and more that this type of family constellation was in danger of nurturing symbiotic illusions about a whole and healthy family without confronting the realities of the relationships between people. That is why I believe it is important to look carefully at the theoretical basis behind the constellations that are carried out.
Since 1998, I have step by step developed my own theory as the basis for the constellation method. It draws on attachment theory (Bowlby 2006 a, b, c, Brisch 2014) and trauma theory (Fischer und Riedesser 1998, Levine 1998, 2011, Herman 2003, Huber 2003, 2013, Putnam 2003). At the same time as I develop my theoretical knowledge, the way I use constellations also changes. I still see constellations as an excellent method for making the psyche visible in a structured way and for illuminating unconscious, very early and dissociated events. Through representatives, the client can see many layers within themselves that can lead to fundamental changes.
I no longer call the procedure "family constellations" or "system constellations" but "trauma constellations." This is because the main focus is always on the trauma that appears behind the client's symptoms, regardless of whether they are of a physical, psychological or social nature.
Since 2009, I have been working with a method I call *"intention constellations". The reason is that I have come to the conclusion that a successful constellation requires the client to formulate his own intention. The intention shows the person's point of view, what moves him, what he has access to in himself, what he wants to open up to and what he does not want to approach. With this method, the intention can be formulated based on the healthy parts of the psyche or based on survival strategies. For example, if someone wants a symptom to disappear, this depends on whether that person is also open to looking at the symptom's cause and function. When that is the case, the intention comes from the healthy parts. If, on the other hand, the client is not interested in what messages the symptom can give, this is a sign that the client is still sticking to a survival strategy.
In the case of an intention constellation, the client first chooses a representative for their intention and positions themselves together with the representative. The dialogue and interaction between the representative of the intention and the client makes visible what it is all about and what change potential the constellation offers the client. There are three general variants:
- The intention, which is at first a survival strategy, changes to a healthy part towards the end of the constellation, i.e. that the client experiences that his healthy structures grow, and that the survival parts gain less power.
- With the help of an intention that comes from the client's healthy parts, access to a traumatized part of the client's psyche becomes possible.
- The intention can help stabilize a healthy state, which has already been established after a previous encounter with the traumatized part.
On the basis of my cleavage model, I have also developed a change model (image 3).
Integration of the split after a trauma
- to open the gate to the trauma feelings
- to reduce the illusions
- to contribute to stabilization and more autonomy
- to strengthen the healthy parts

Image 3: The change model for multigenerational psychotraumatology.
Constellations of intention and salutogenesis
Meaningful, understandable and manageable are the main concepts in the Salutogenesis model (theory of what promotes good health) by Aaron Antonovsky (Antonovsky 1997). All three dimensions are also found in my model for the healthy psychological structures. Only if the psyche fulfills its proper function and gives us access to the outer and inner reality, are we in the healthy parts of the psyche. When, on the other hand, we are governed by the trauma or survival parts, reality is largely toned down, which increases the risk of further traumatisation.
Our experiences are especially significant when they are connected to emotions. If we are separated from our feelings, much becomes meaningless to us, and we will experience an inner emptiness. Based on the inner emptiness, we can also do things that are harmful to us, without us being aware of it. Trauma survivors may try to fill this void with addictions, such as drugs, and the addiction will in turn lead to further traumatization and more disease symptoms.
When we talk about understanding something in a cognitive way, here too it is clear that only a healthy psyche can realize what is really happening. The traumatized parts, on the other hand, do not try to understand what is happening (partly very purposefully), in order to shield themselves from anxiety and pain. Instead, they create a dream world in which they try to live. They accept the loss of reality in order to avoid being confronted with memories of the trauma. It is also the trauma survivor parts that feel relieved when the symptoms, which they themselves create, are not scrutinized to find causes, but instead are labeled as illness. In this way, responsibility for one's own health is delegated to experts, and one can assume a victim role in relation to one's own illnesses.
Manageability is the practical side of a healthy psyche. We see the possibilities we have for concrete actions. These actions are targeted and solve the problems where this is possible. Only the healthy part is able to deal with the realities of trauma. Also at this level, the trauma survivors follow a different logic: They see opportunities for action where there are none, and they overlook the opportunities that exist to solve the problems. They are either too optimistic or too pessimistic. They also do not see the opportunities to recover from the trauma or to prevent new traumas from occurring. They are convinced that the trauma does not exist, at least not in themselves.
Through the constellation method, psychic structures can be seen in all their complexity. Therefore, it is also possible to examine in detail whether the measures that are put in place can be helpful, and which measures lead a person even deeper into a psychological split. Many times it has been shown in constellations that what clients have previously thought was health-promoting, was just another new survival strategy to be able to tolerate the consequences of trauma better, or to compensate for them.
All experience with therapy to date shows that the greatest health-promoting potential lies in reintegrating separated psychic structures. This is how you can make the cognition and emotions of a traumatized person no longer stand in opposition to each other. On the contrary, they can complement each other in a meaningful way.
The main reason why clients seek out my psychotherapeutic practice is that they have been exposed to trauma. Often these experiences go back a long way in their biography, often even going back to the time before their birth. Here I use the term "early trauma" (Ruppert 2014). Striking physical and psychological features (symptoms) are therefore not an independent illness. It is another indication that this person has experiences in life that have not been processed in a good way. If, for example, a child has symptoms, it is not necessarily the case that there is something wrong with the child. It may just as well be that the child lives in unhealthy relationships. It often turns out that when the mother or father works on their own traumas, the symptoms of illness in the child will also disappear.
Good health cannot therefore be defined as being without symptoms. In my opinion, good health is based on healthy structures in a living organism. It is a result of what we eat, physical activity and primarily psychological programs that we use to design and experience our interpersonal relationships. Denying and repressing do not promote salutogenesis. Working purposefully, consistently and continuously through already experienced trauma and getting out of traumatizing relationships is, on the other hand, beneficial for health.
If we humans could also stop mutually traumatizing each other (for example through wars, violence in relationships or in parent-child relationships), that would be the greatest contribution we could make to the health of humanity.
*The methodology within the "intention constellations" method has been changed since Ruppert wrote this article, and the new methodology will be presented at the Trauma Conference.